When Science Meets the Sacred: Bureaucracy vs. Healing
Two rejection letters from a world that wants 3,000 years of healing reduced to one molecule, one receptor, and one placebo jaguar.

I'm a neuroscience geek. Show me 5-HT2A receptor binding data and I get genuinely excited. Mention REBUS, cytokines, microglia, or critical-period reopening and you've got my attention. The renaissance of psychedelic research over the past two decades (and its explosion in the past ten years) has been nothing short of extraordinary. And I want more of it. More mechanisms, more indications, more rigorous science unlocking how these compounds heal minds that conventional medicine often cannot touch.
But you can't always get what you want.
The FDA's rejection of Lykos's MDMA therapy application in 2024 (and their belated CRL in 2025) highlights just how hard it is to fit psychedelic healing into existing regulatory framework, even with solid clinical data. Meanwhile, there's growing excitement around "trip-less" psychedelics: compounds engineered to deliver neuroplasticity without the subjective journey. While that concept gives me great agita (to put it mildly), that might be invaluable for people who can't tolerate a full psychedelic experience. Some healing is always better than none.
But research keeps showing that mystical experience scores are among the strongest predictors of long-term outcomes. The subjective journey, meaning the ineffable, transformative experience, isn't an inconvenient side effect. It may be the medicine itself. Even Osmond's 1957 coinage "psychedelic" (mind-revealing) suggests that the revelation, not just the neurochemistry, might be the point.
So here's the paradox: the most effective therapies struggle for approval precisely because they alter consciousness. Meanwhile the pharmaceutical solution is to eliminate the consciousness-altering part entirely. Engineer away the "trip," and you may also be engineering away the heart of the healing.
This tension got me wondering: How would Dr. Shaman fare in front of an IRB? What happens when we try to force ancient healing wisdom through the machinery of modern drug approval? What would it look like if a traditional shaman tried to get FDA approval for ceremonies that have safely healed humans for millennia?
What follows is that bureaucratic collision: two rejection letters that illustrate how we think about healing, consciousness, and what counts as "real" medicine. (For another take on this, see Herbalism for the Woo-Allergic.)
And consider this: Dr. Shaman's protocol probably is incredibly sophisticated. Indigenous healers account for individual constitution, community dynamics, seasonal cycles, and dozens of other variables that our reductionist paradigm literally cannot see. The tragedy isn't in their methods. It's in our inability to recognize valid therapeutic frameworks when they don't fit our forms.
In our rush to extract active ingredients and optimize outcomes, what essential medicine are we leaving behind? Nothing bad ever came from refining coca leaf into cocaine, after all. And how many valid healing approaches do we reject simply because they can't be reduced to isolated variables?
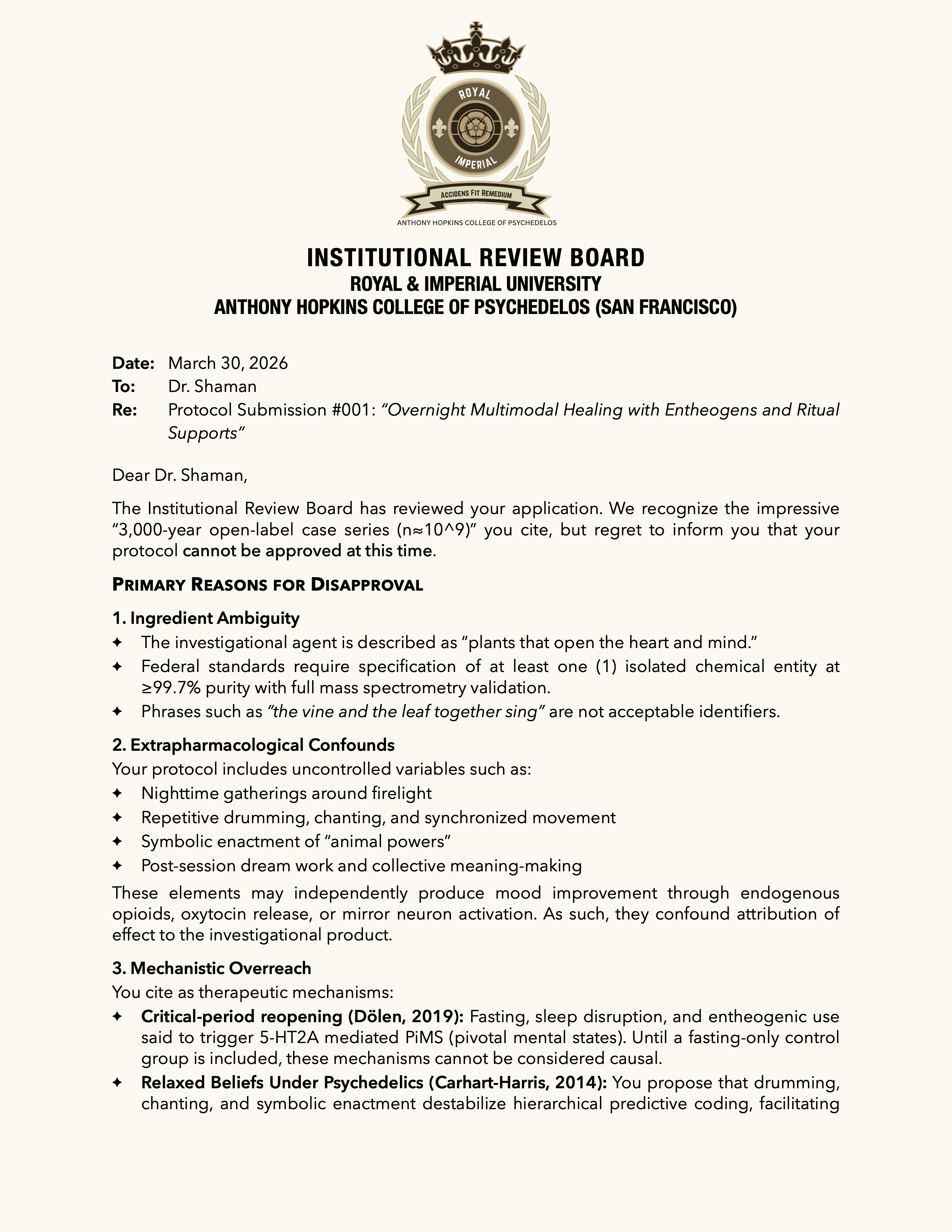
Institutional Review Board
Royal & Imperial University
Anthony Hopkins College of Psychedelos (San Francisco)
Date: March 30, 2026
To: Dr. Shaman
Re: Protocol Submission #001 — "Overnight Multimodal Healing with Entheogens and Ritual Supports"
Dear Dr. Shaman,
The Institutional Review Board has reviewed your application. We recognize the impressive "3,000-year open-label case series (n≈10^9)" you cite, but regret to inform you that your protocol cannot be approved at this time.
Primary Reasons for Disapproval
1. Ingredient Ambiguity
- The investigational agent is described as "plants that open the heart and mind."
- Federal standards require specification of at least one (1) isolated chemical entity at ≥99.7% purity with full mass spectrometry validation.
- Phrases such as "the vine and the leaf together sing" are not acceptable identifiers.
2. Extrapharmacological Confounds Your protocol includes uncontrolled variables such as:
- Nighttime gatherings around firelight
- Repetitive drumming, chanting, and synchronized movement
- Symbolic enactment of "animal powers"
- Post-session dream work and collective meaning-making
These elements may independently produce mood improvement through endogenous opioids, oxytocin release, or mirror neuron activation. As such, they confound attribution of effect to the investigational product.
3. Mechanistic Overreach You cite as therapeutic mechanisms:
- Critical-period reopening (Dölen, 2019): Fasting, sleep disruption, and entheogenic use said to trigger 5-HT2A mediated PiMS (pivotal mental states). Until a fasting-only control group is included, these mechanisms cannot be considered causal.
- Relaxed Beliefs Under Psychedelics (Carhart-Harris, 2014): You propose that drumming, chanting, and symbolic enactment destabilize hierarchical predictive coding, facilitating belief revision. The IRB considers this speculative without a validated fMRI-based biomarker of "belief unweighting."
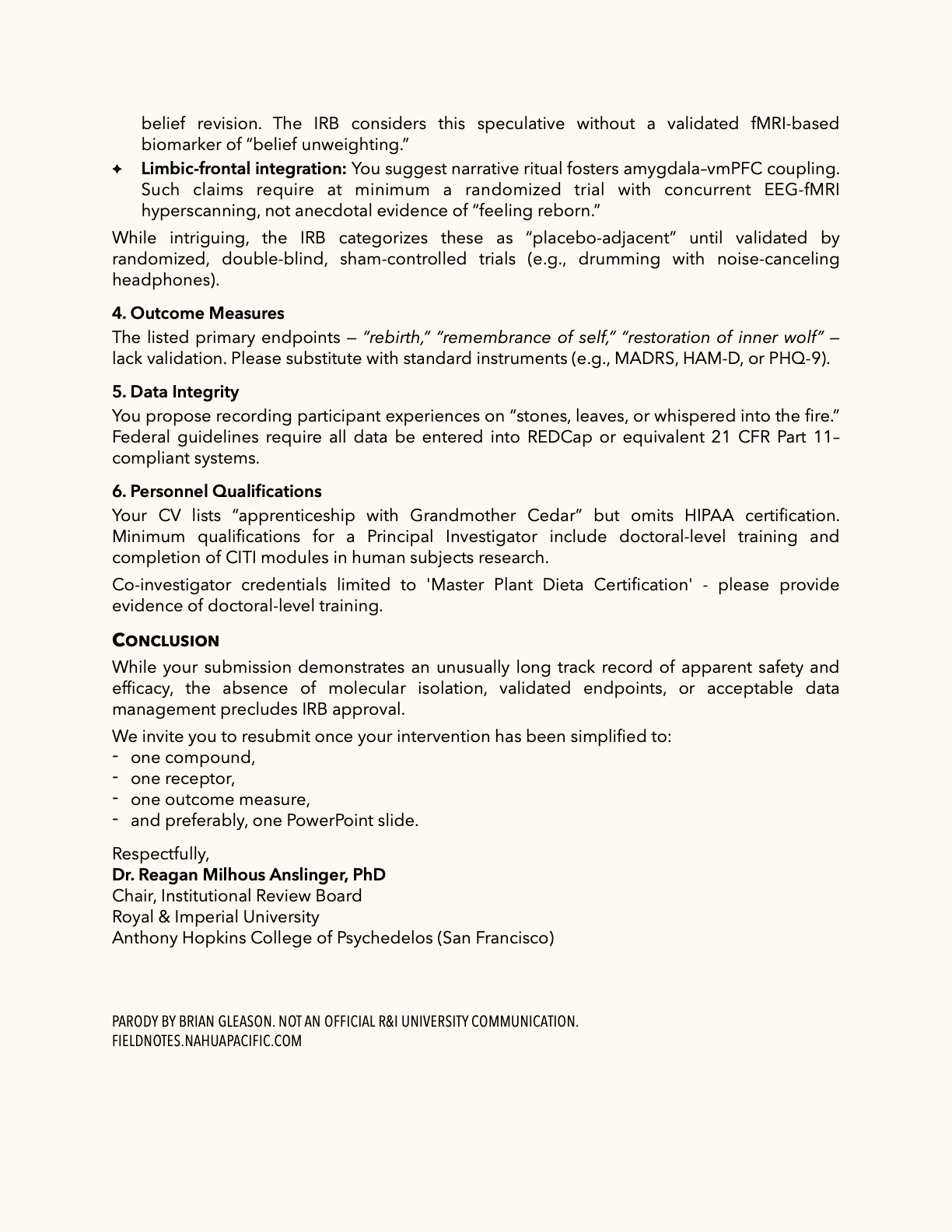
- Limbic-frontal integration: You suggest narrative ritual fosters amygdala–vmPFC coupling. Such claims require at minimum a randomized trial with concurrent EEG-fMRI hyperscanning, not anecdotal evidence of "feeling reborn."
While intriguing, the IRB categorizes these as "placebo-adjacent" until validated by randomized, double-blind, sham-controlled trials (e.g., drumming with noise-canceling headphones).
4. Outcome Measures The listed primary endpoints — "rebirth," "remembrance of self," "restoration of inner wolf" — lack validation. Please substitute with standard instruments (e.g., MADRS, HAM-D, or PHQ-9).
5. Data Integrity You propose recording participant experiences on "stones, leaves, or whispered into the fire." Federal guidelines require all data be entered into REDCap or equivalent 21 CFR Part 11–compliant systems.
6. Personnel Qualifications Your CV lists "apprenticeship with Grandmother Cedar" but omits HIPAA certification. Minimum qualifications for a Principal Investigator include doctoral-level training and completion of CITI modules in human subjects research.
Co-investigator credentials limited to "Master Plant Dieta Certification" — please provide evidence of doctoral-level training.
Conclusion
While your submission demonstrates an unusually long track record of apparent safety and efficacy, the absence of molecular isolation, validated endpoints, or acceptable data management precludes IRB approval.
We invite you to resubmit once your intervention has been simplified to:
- one compound,
- one receptor,
- one outcome measure,
- and preferably, one PowerPoint slide.
Respectfully, Dr. Reagan Milhous Anslinger, PhD Chair, Institutional Review Board Royal & Imperial University Anthony Hopkins College of Psychedelos (San Francisco)
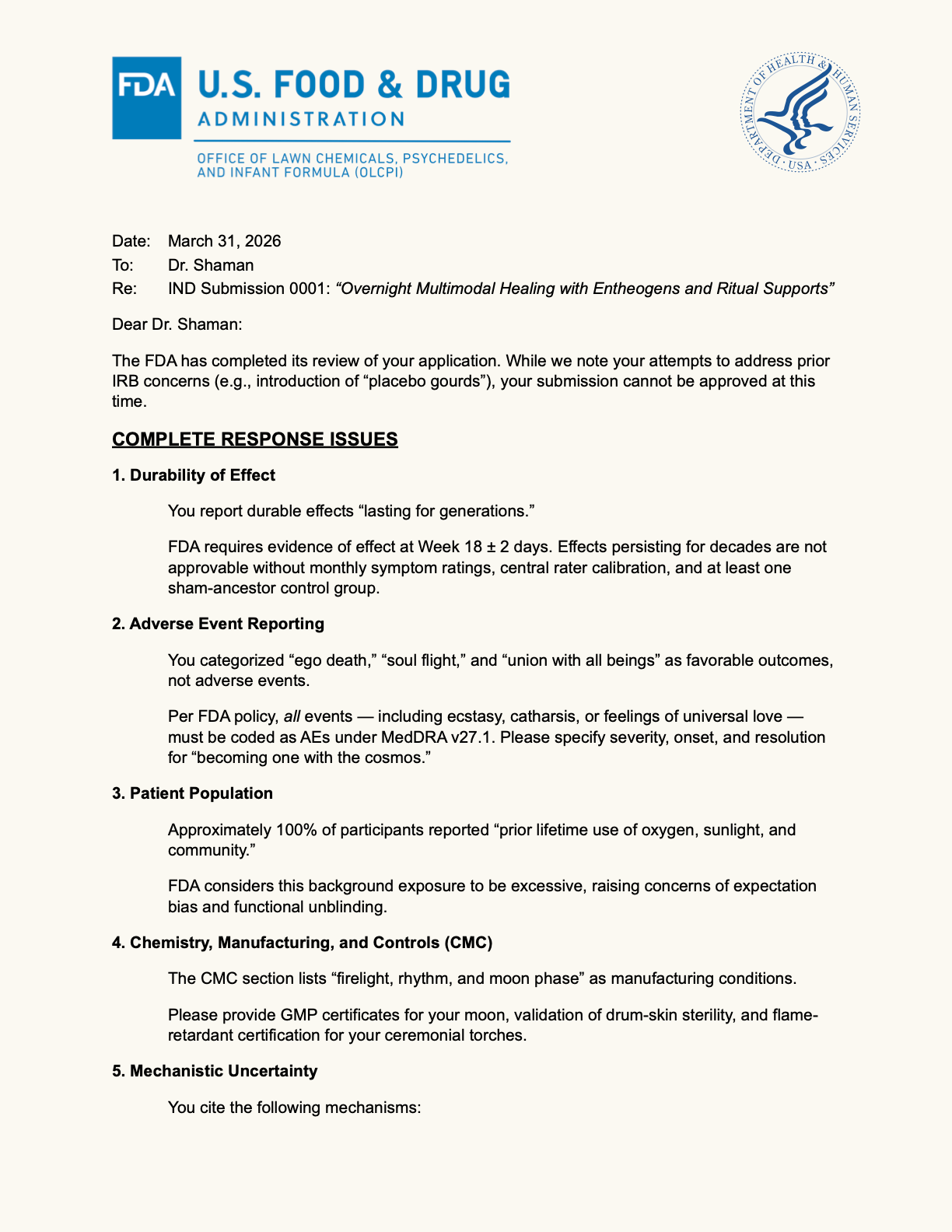
U.S. Food and Drug Administration
Office of Lawn Chemicals, Psychedelics, and Infant Formula (OLCPI)
Date: March 31, 2026
To: Dr. Shaman
Re: IND Submission #0001 — "Overnight Multimodal Healing with Entheogens and Ritual Supports"
Dear Dr. Shaman,
The FDA has completed its review of your application. While we note your attempts to address prior IRB concerns (e.g., introduction of "placebo gourds"), your submission cannot be approved at this time.
Complete Response Issues
1. Durability of Effect
- You report durable effects "lasting for generations."
- FDA requires evidence of effect at Week 18 ± 2 days. Effects persisting for decades are not approvable without monthly symptom ratings, central rater calibration, and at least one sham-ancestor control group.
2. Adverse Event Reporting
- You categorized "ego death," "soul flight," and "union with all beings" as favorable outcomes, not adverse events.
- Per FDA policy, all events — including ecstasy, catharsis, or feelings of universal love — must be coded as AEs under MedDRA v27.1. Please specify severity, onset, and resolution for "becoming one with the cosmos."
3. Patient Population
- Approximately 100% of participants reported "prior lifetime use of oxygen, sunlight, and community."
- FDA considers this background exposure to be excessive, raising concerns of expectation bias and functional unblinding.
4. Chemistry, Manufacturing, and Controls (CMC)
- The CMC section lists "firelight, rhythm, and moon phase" as manufacturing conditions.
- Please provide GMP certificates for your moon, validation of drum-skin sterility, and flame-retardant certification for your ceremonial torches.
5. Mechanistic Uncertainty You cite the following mechanisms:
- PiMS-induced critical period reopening (Dölen, 2019). Requires a fasting-only, sleep-deprivation-only, and jaguar-costume-only arm to isolate effects.
- Relaxed Beliefs Under Psychedelics (Carhart-Harris, 2014). Until "belief unweighting" can be measured on a 7-point Likert scale, these claims remain exploratory.
- Amygdala–vmPFC coupling through chant. Please submit simultaneous PET-MEG-EEG hyperscanning during synchronized drumming, ideally under red light.
6. Outcome Measures
- The primary endpoints — "rebirth," "restoration of inner wolf," "remembrance of self" — are not validated instruments.
- FDA recommends MADRS, HAM-D, or the Beck "Inner Wolf" Inventory if developed.
7. Data Capture
- Transition from "whispering into the fire" to "goat vellum" is noted.
- However, 21 CFR Part 11 requires an audit trail. Unless the fire can produce timestamped metadata, these data remain noncompliant.
Conclusion
Your submission demonstrates impressive longevity of use (n≈10^9, ~3,000 years). However, without evidence of durable effect at Week 18, validated endpoints, GMP-certified moonlight, and MedDRA-coded universal love, FDA cannot approve this application.
We recommend resubmission once your intervention has been reduced to:
- one molecule,
- one receptor,
- one outcome measure,
- and one placebo jaguar.
Respectfully, Dr. Ignatius K. Nullman, JD, MPH, PhD, MBA, CPR (Expired)
Director, Office of Lawn Chemicals, Psychedelics, and Infant Formula (OLCPI) U.S. Food and Drug Administration
fieldnotes.nahuapacific.com | nahuapacific.com | nahuaorigins.com

Essays on treatment resistance, altered states, and the conditions under which change becomes possible.
Subscribe