The Three-Level Collapse
Why you can't think, rewire, or want your way out (SLM 6 of 10)
This is the sixth essay in our ten-part series on the Signal Loss Model. In SLM 1, we showed that depression and anxiety are symptom clusters emerging from shared biological substrates, not discrete diseases. In SLM 2, we explained how the brain's simulation machinery decouples from reality when environmental constraints disappear. In SLM 3, we showed why the same architecture collapses differently depending on how constraint is applied across the lifespan. In SLM 4, we detailed how chronic stress drives an inflammatory cascade that suppresses neuroplasticity, biologically freezing maladaptive patterns. In SLM 5, we examined how sustained cortisol elevation dismantles the brain's reward system, collapsing the motivational pull that makes anything feel worth pursuing. Here, we ask the question those five essays have been building toward: what happens when all three mechanisms are running simultaneously, and what it actually takes to stop them.
One Year Later
Elena tried therapy.
She found a good one. A serious clinician, psychodynamically trained, familiar with high-functioning presentations. They worked together for six months. Elena was a model patient: articulate, introspective, reliable. She was, it turned out, extraordinarily good at this.
The insights came steadily. The childhood architecture that had fed her drive. The way performance had substituted for safety at an age when she hadn't known the difference. The key moments when the machine had been assembled and why. She could name them, date them. Her therapist was skilled. Elena was skilled. The sessions had the particular energy of two intelligent people doing serious work together.
In month six, she was driving home from a session, a good one, another genuine breakthrough, when something new crystallized. She pulled over. She sat with it.
Six months. How many insights is that?
She could not identify a single thing in her life that had actually changed.
She went back the following week and said so. Her therapist suggested they adjust the approach. They did. Three months later nothing had changed, and Elena concluded that the problem must be the therapist. She found another. Then another.
She was still looking for the insight that would finally be enough.
James made a list.
This was not unusual. He had run a logistics company for twenty-two years on the strength of lists, plans, and the disciplined conversion of both into outcomes. He knew how to identify an opportunity, map a path, and execute. The exit had confirmed it, at a number with a lot of zeros.
Eighteen months later, sitting in an office he'd built for the next chapter, he made a list of what that chapter might look like. Seven items. Solid ones. He still knew how to think. He read the list back. He waited.
Nothing pulled.
He told himself he needed more time. He refined the list. He did research. Three weeks later he had a genuine plan: well-structured, realistic, the kind of thing he would have funded without hesitation from the other side of the table.
He put it in a drawer. He wasn't sure why.
His daughter called that week. His grandson was on a school break, did he want to come? He did. He drove four hours, and for two days it was genuinely good. His grandson was seven and relentless and funny in the specific way that seven-year-olds are funny when they don't know they're being funny. James was present for it. He felt something that resembled what he was looking for.
He drove home. By the time he pulled into his driveway, it was already gone.
He opened the drawer. Read the plan again. This time it felt like someone else had written it. The plan was competent and well-reasoned. And James felt completely inert. He closed the drawer.
Maybe it wasn't the right idea. He opened a new document. He would think of something better. He was still someone who could think of something better.
The new document stayed open for eleven days. He added four lines. He told people he was exploring options.
He wasn't exploring. He was waiting for something to feel like it was worth exploring. It was a distinction he hadn't yet found the words for, and wouldn't have shared if he had.
Priya, who had always enjoyed a contemplative practice, went deeper.
She had meditated for thirty years. She knew how to sit. She knew how to breathe. She knew that difficult states were not permanent and that awareness itself was the ground beneath the weather. She trusted the practice.
She added a daily sitting. Extended her existing practice. Attended a silent retreat in the mountains for ten days.
She came back clear, quiet, and temporarily at peace. It lasted not quite five days. Then the stillness faded, the institutional demands reasserted themselves, and the familiar hollow returned. Not dramatically. Just the particular tedium of a tide she now recognized. She had learned to observe the emptiness. She had not escaped it.
"I think I've been meditating at it," she told a colleague afterward, "rather than through it."
Three intelligent people. Three well-chosen interventions. Three failures.
Not spectacular failures. These aren't people who spiral visibly or collapse dramatically. The failures are internal, which in some ways makes them worse. Elena is still in therapy. James still has the list. Priya still meditates every morning. From the outside, they look like people doing everything right.
From the inside, something more frightening is happening. Not crisis. They would almost welcome crisis, because crisis implies a bottom, and a bottom implies the possibility of up. What they're living with is more like a slow, private recalibration of expectations. The question that doesn't get spoken aloud, that surfaces at 3am or on the drive home or in the eleven seconds after the grandkids leave: Is this just what it's going to be now?
They have each run headlong into the same wall, from three different directions.
The wall has a name. And understanding why it's there is the only way to understand what it would actually take to get through it.
The System, Not the Symptoms
Here is what the previous essays have established on their own:
In SLM 2, we showed that Elena's simulation machinery (the cognitive architecture that made her a senior partner) has decoupled from reality. Without concrete external constraints providing error-correction, it runs recursive loops: threat modeling, performance comparison, abstract self-interrogation. The loops are self-reinforcing. They generate chronic psychological stress. And crucially, they generate it continuously, because there is no external reality-check to interrupt them.
In SLM 4, we showed that James's brain has been biologically locked in place. Months of untethered simulation running threat loops have produced a persistent inflammatory state that has suppressed the neuroplasticity machinery. The biological capacity for pattern change (the cellular infrastructure that would allow experience to rewire neural architecture) has been chemically downregulated. He cannot rewire because the rewiring apparatus is offline.
In SLM 5, we showed that Priya's reward system has been systematically dismantled. Decades of sustained cortisol exposure have stripped D2 receptor density from her striatum. The wanting machine (the motivational signal that makes things feel worth pursuing) has gone quiet. She can see what might be worth doing. She cannot generate the neurochemical pull to move toward any of it.
Each essay used one person to foreground one mechanism. The mechanisms don't actually observe that boundary. Three mechanisms. Three people. Three different presentations of the same underlying failure.
But here is what the previous essays, by design, left implicit: these three mechanisms are not parallel processes happening to share the same host. They are a single self-reinforcing system. Each level worsens the other two. Each failed recovery attempt deepens all three. And together, they converge on a stable pathological equilibrium. Not a comfortable one. But stable, because every exit route is blocked by one of the other levels.
This is why Elena's therapy didn't work. This is why James's new goals made things worse. This is why Priya's meditation brought temporary relief but not recovery.
This is the Three-Level Collapse.
Why Elena's Therapy Failed
The logic of psychotherapy, at least in its cognitive and psychodynamic forms, is this: if you can understand the pattern, you can change it. Insight produces leverage. Leverage produces behavioral change. Behavioral change, consolidated over time, produces new neural architecture.
This logic is correct. Under normal biological conditions, it works. Understanding how a pattern formed and why it persists does create the cognitive purchase needed to begin reorienting it. Talk therapy has an evidence base. Its mechanism is real.
The mechanism requires a functioning substrate.
What Elena's therapy didn't account for, and what almost no clinical protocol adequately accounts for in this population, is that the biological machinery for change was not available to her. The neuroplasticity suppression we detailed in SLM 4 is not a metaphor for being "stuck." It is a measurable reduction in BDNF expression and synaptic plasticity driven by cytokine activity (Miller & Raison, 2016). The cellular infrastructure that converts insight into rewired neural patterns has been chemically downregulated.
Elena could generate insight without limit. She could understand her patterns with surgical precision. The machinery that would translate that insight into lasting change was offline.
Insight without plasticity is archaeology, not renovation. You can map the structure of an old building with extraordinary detail. You cannot change it if the construction equipment won't start.
And here is where the cascade deepens: because therapy wasn't working, Elena's simulation machinery, the untethered pattern-matcher running in background, added it to the threat model. The thing that was supposed to fix this isn't working. Which means either the therapist is wrong, or I am beyond fixing. The loops didn't stop. They incorporated the failure.
Cortisol elevated further. Inflammation tightened its grip. Recovery became biologically harder.
The intervention intended to help had been metabolized by the system into additional evidence of threat.
Why James's Plans Went into the Drawer
James wasn't running a therapeutic protocol. He was doing what he had always done: identify something worth pursuing, build a plan, execute. The approach had worked for twenty-five years. He had no reason to believe the approach was the problem.
The problem was what happened in the gap between the plan and the doing.
The reward system James had relied on his entire career runs on dopaminergic signaling. Specifically, it drew on the anticipatory pull that makes a credible plan feel like something worth moving toward. That signal is generated and received by D2 receptor infrastructure that twenty-five years of sustained cortisol exposure had quietly stripped down (Treadway & Zald, 2011). The plan was sound. The neurochemical response that should have followed (the forward lean, the energy of early commitment) didn't come. Or came briefly and dissolved before it could generate momentum.
So he refined the plan. Made it better. More realistic, better-structured, the kind of thing he would have jumped on back in the day. Read it back. Waited.
Still nothing.
What did fire, reliably, was the performance architecture. The moment any plan reached the threshold of something real, as in something that could succeed or fail, the simulation machinery generated its habitual response: threat modeling, comparison, projection into uncertain futures. Cortisol elevated. D2 receptors, already depleted, were further suppressed. The planning that was meant to restore a sense of forward motion was instead re-administering the stress chemistry that had caused the depletion.
James's grandson provided a flicker of hope, genuine and brief. But brief is the operative word. The reward system could still fire. It just couldn't sustain. Nothing held long enough to become momentum.
Each attempt left him slightly further from believing the next one would be different. Each failure to feel what he expected to feel became evidence in a case his own mind was quietly building: that he had become someone who couldn't follow through. That the edge was gone. That the plan-in-the-drawer, the inertia, the desert of identical days was all that would remain.
He wasn't lazy. He wasn't weak. The system, in its broken way, was protecting itself from further damage. The drawer was not failure. It was biology.
Why Priya's Meditation Brought Relief But Not Recovery
This one is the hardest to explain, because meditation does work: in specific ways, for specific mechanisms, under specific biological conditions. The autonomic regulation that contemplative practice develops is genuinely relevant to the Signal Loss Model. Parasympathetic activation reduces cortisol. Vagal tone supports the cholinergic anti-inflammatory pathway. Mindfulness-based interventions have documented anti-inflammatory effects (Bower & Irwin, 2016). Priya was not wrong to go deeper.
But there is a difference between relief and recovery. And the gap between them, in Priya's case, is the simulation machinery itself.
The untethered simulation loop, the cognitive architecture running recursive threat models and abstract self-interrogation, is not quieted by observing it. Observation is metacognitive. The loops are lower-level. They continue beneath the watching, the way a river continues beneath a bridge. The bridge does not affect the river.
What meditation gave Priya, at the retreat, was a temporary environmental constraint: structure, silence, direction, the absence of her institutional context. The simulation machinery, deprived of its normal inputs, slowed. The parasympathetic state generated genuine autonomic relief. She felt it as clarity.
When she returned to her institutional context, the inputs returned. The loops resumed. The constraint that had organized the nervous system dissolved back into the ordinary day.
Priya had experienced the relief that constraint produces. But the retreat was the constraint, not the meditation. The practice she brought home was separated from the environment that had made it effective.
And here the inflammatory lock-in tightened the vise: the brief parasympathetic window the retreat opened (the window during which neuroplastic change might have been possible) closed without new patterns being installed. The system returned to its prior stable state. Which is, biologically, exactly what stable states do.
The Closed Loop
We now have enough to name what's actually happening. This is not three bad things occurring in the same person. It is a closed system of mutual reinforcement.
The simulation machinery generates chronic psychological stress. That stress drives cortisol elevation and cellular damage that feeds the inflammatory cascade. The inflammatory cascade suppresses neuroplasticity, making the simulation patterns biologically durable. They are harder to exit because the tissue-level machinery for change has been downregulated. The same inflammatory state drives cytokine interference with dopamine synthesis and D2 receptor availability, collapsing incentive salience. Without external motivational pull, the simulation machinery, deprived of concrete targets, turns further inward, generating more abstract loops, more unresolvable threat modeling, more cortisol. Which deepens the inflammation. Which further suppresses plasticity and reward.
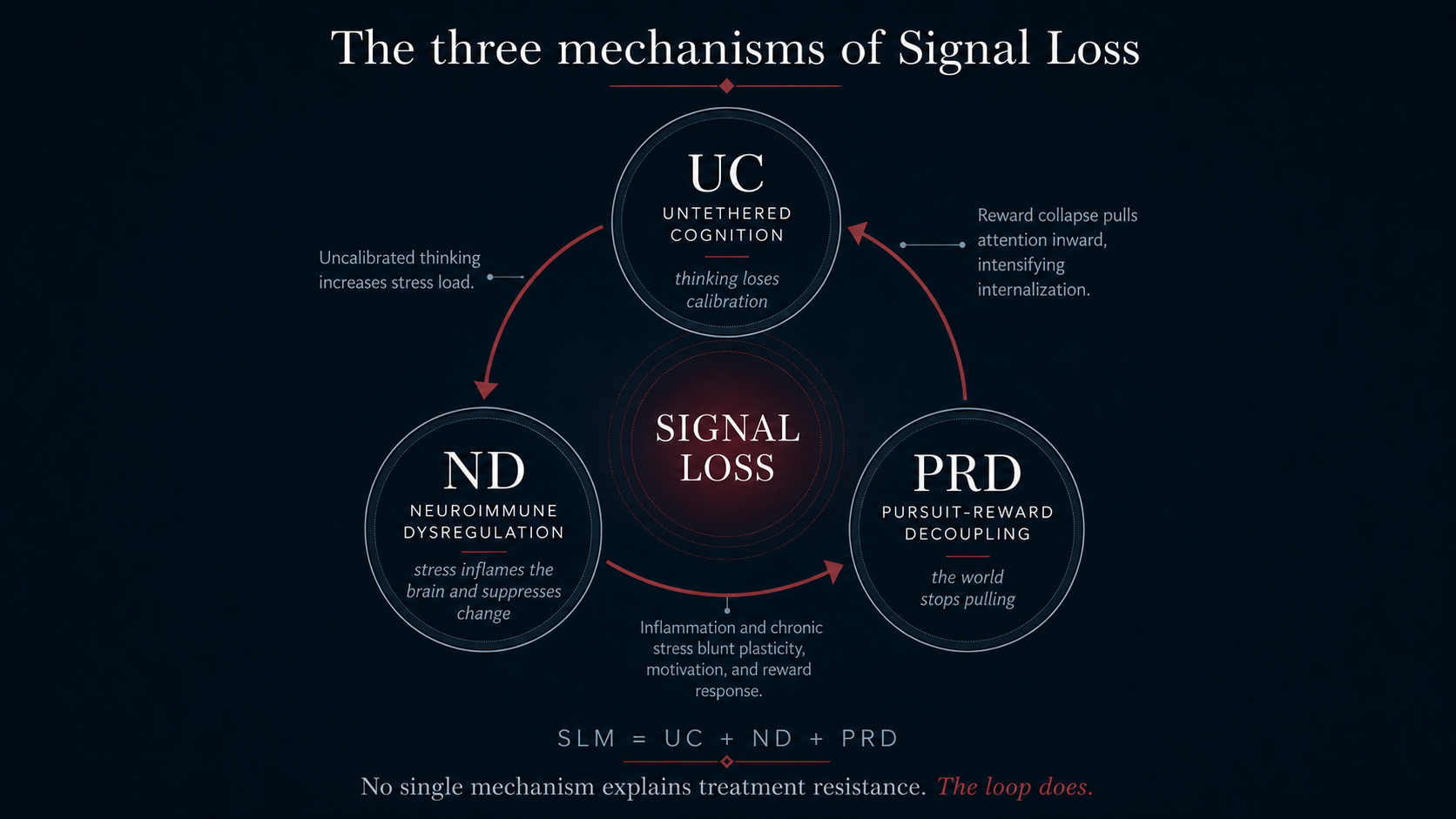
The loop is not metaphorical. Each of these arrows is a documented biological mechanism. The self-reinforcement is not a tendency or a risk factor. It is the system's operating logic.
This is why standard single-level interventions fail. Each one can effectively address the level it is aiming for. But meanwhile the other two levels actively absorb and neutralize the intervention. The system is not passively resistant. It is actively stabilizing. It converts recovery attempts into threat signals and uses them to maintain equilibrium.
The system is not a disease. It is a very effective maintenance mechanism, running exactly as designed, in exactly the wrong conditions.
What Stability Actually Means
Pause on the word "stable."
When we say the Three-Level Collapse produces a stable equilibrium, it sounds like a verdict. It isn't. Stability is a systems concept, not a moral one. A stable state is one that returns to equilibrium after perturbation. It says nothing about whether the equilibrium is desirable.
A ball at the bottom of a bowl is in stable equilibrium. Push it, it returns. But stability is a function of the bowl's shape, not of destiny. Change the bowl, change the forces that are maintaining the equilibrium, and the stable state becomes unstable. The ball can move.
For Elena, James, and Priya, what looked like three separate treatment failures was actually the system demonstrating its stability. Each intervention pushed from one direction. The other two levels pushed back. The system returned to center.
This is important clinical information, not a reason for despair. A system this coherent fails coherently. It can be understood. It can, in principle, be disrupted. But only by interventions that address all three levels simultaneously.
The perturbation has to exceed the restoring force. The bowl itself has to change.
You cannot think your way out when the neuroplasticity required to rewire the thinking machinery is suppressed by inflammation.
You cannot rewire your way out when the reward signal that would make new patterns feel worth consolidating can no longer be received.
You cannot want your way out when the simulation loops generating the wanting are untethered from the concrete reality that could recalibrate them.
But this is not a statement about impossibility. It is a statement about conditions. The biology defines the problem. It does not automatically specify the solution.
What Would Actually Work
We're going to be careful here, because SLM 7 addresses this question in detail. Specifically, we address the epistemological question of how to choose interventions without falling into the magical thinking that characterizes most of what passes for transformation in this space.
But the logic of the Three-Level Collapse points toward certain requirements, regardless of specific modality.
Any intervention capable of disrupting this system would need to do something none of Elena, James, or Priya's attempts managed: address all three levels at once, in a manner that doesn't allow the unaddressed levels to neutralize the addressed one.
That means the first move cannot be understanding. Elena understood her patterns with preternatural accuracy. Understanding didn't fail because it was wrong. It failed because the simulation machinery incorporated each insight into the next recursive loop. The pattern absorbed the analysis of the pattern. Insight without plasticity is not incomplete therapy. It is the system metabolizing the intervention.
The first move cannot be planning and doing. James built credible, well-structured plans and attempted to execute them through sheer discipline. The plans didn't fail because they were misguided. They failed because the reward system that would have made any plan feel worth pursuing had been neurochemically dismantled. Discipline without motivational signal is not a willpower problem. It is effort aimed at a receptor system that can no longer receive it.
And the first move cannot be observing. Priya watched the patterns from above with thirty years of contemplative skill. The observation didn't fail because the practice was shallow. It failed because the loops she was observing run beneath the level that observation reaches. Awareness without biological disruption of the underlying state is not insufficient practice. It is a bridge that does not touch the river.
The first move has to operate at the level of the biological state itself: resetting the autonomic conditions that are feeding all three mechanisms simultaneously. Before insight can be useful, the tissue-level substrate for insight-driven change has to be restored. Before new patterns can be installed, the system has to be in a biological state that allows installation. Before motivation can be rebuilt, the stress physiology that is systematically dismantling the reward architecture has to be interrupted.
The biological reset is not the intervention. It is the precondition for the intervention.
And the integration that follows the disruption, the structured installation of new constraints during the window when the system is biologically capable of rewiring, is not optional. It is the mechanism. Without it, the system returns to its prior stable state, because stable states are what systems do.
This is the question SLM 7 takes up: how do you choose interventions without magical thinking when you understand that the system is operating as a system, and that insight about the problem is not the same as the biological conditions required to solve it?
The answer exists. But it requires thinking about epistemology before modality. Understanding how you know something works, before deciding that it will.
For Elena, James, and Priya
Elena's therapy wasn't wrong. Her therapist was good, her insight was real, her effort was genuine. The understanding was real. The biological substrate for acting on it had been suppressed before she walked through the door. She has been trying to renovate a house with the construction equipment locked in a shed she doesn't have the key to.
James's new goals weren't misguided. Behavioral activation is a legitimate and well-supported approach (Jacobson et al. 2001). The discipline was there. Each attempt at a new target was re-administering the cortisol that depleted the very receptor infrastructure those targets were supposed to rebuild. He has been trying to refill a tank that the filling mechanism was simultaneously draining.
Priya's practice wasn't ineffective. The relief she experienced at the retreat was real, a genuine autonomic shift with documented biological correlates. The practice was sufficient. What worked, though, was the retreat itself: the silence, the structure, the removal of her institutional life. The practice was what she did inside that container, and the container was the one thing she couldn't carry home. She has been heating a room with the door open, and wondering why it never holds the warmth.
None of them were doing it wrong. All of them were incomplete.
The Three-Level Collapse is not a description of broken people. It is a description of a coherent system, running its logic faithfully, in an environment that has removed the inputs it was designed to receive.
You cannot fix a systems problem with a component solution.
But you can fix it.
In SLM 7: Choosing Interventions Without Magical Thinking, we turn to the epistemological question the model demands: how do you evaluate an intervention when the system it's targeting is this complex, when sequence matters more than modality, and when the field offering solutions ranges from rigorous science to elaborate nonsense, often wearing the same vocabulary?
References
Bower, Julienne E., and Michael R. Irwin. 2016. “Mind–Body Therapies and Control of Inflammatory Biology: A Descriptive Review.” Brain, Behavior, and Immunity 51 (January): 1–11.
Jacobson, Neil S., Christopher R. Martell, and Sona Dimidjian. 2001. “Behavioral Activation Treatment for Depression: Returning to Contextual Roots.” Clinical Psychology: Science and Practice (United Kingdom) 8 (3): 255–70.
Miller, Andrew H., and Charles L. Raison. 2016. “The Role of Inflammation in Depression: From Evolutionary Imperative to Modern Treatment Target.” Nature Reviews. Immunology 16 (1): 22–34.
Treadway, Michael T., and David H. Zald. 2011. “Reconsidering Anhedonia in Depression: Lessons from Translational Neuroscience.” Neuroscience and Biobehavioral Reviews 35 (3): 537–55.

Essays on treatment resistance, altered states, and the conditions under which change becomes possible.
Subscribe